For most women, health and wellbeing are influenced by the reproductive hormones oestrogen, progesterone and testosterone.
This starts when young girls enter puberty in late childhood/early teens and continues into the post-menopausal period and beyond. The degree of fluctuations and their impact vary between individuals and the stage of life they are at. This is particularly the case around puberty and the perimenopause, when hormone fluctuations can be quite marked, with a more stable period in between during which women are at their most fertile. These erratic hormone changes can cause a variety of symptoms. Although these symptoms can occur at different life stages, for the purposes of this article we will focus on the perimenopausal period.
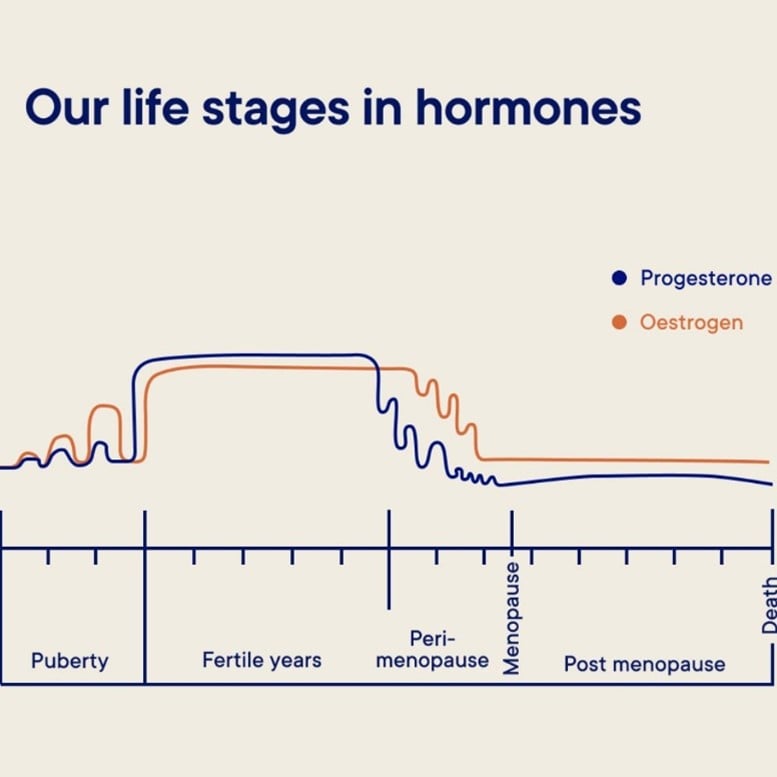
Fig 1: Our Life stages in hormones. Source: Your Lifestyle Medics
What is the perimenopause?
Menopause refers to the time in every woman’s life when her periods stop, and the ovaries lose their reproductive function. Menopause is defined as 12 consecutive months without a menstrual period, provided there is no other medical cause, if over 50 years old, and 24 months if under 50. The average age of ‘natural’ menopause in the UK is 51 years. However, the 10 years either side of this can be a time of hormonal fluctuations when the ovaries are slowly beginning to ‘wind down’; this is called the perimenopausal period.
In a small number of cases, women can become menopausal in their 30s or even younger; this is called ‘premature menopause’ or ‘premature ovarian insufficiency’. Equally, surgery or cancer treatment can lead to a more sudden menopause.
What are the symptoms of perimenopause?
Due to the gradual reduction in oestrogen and the wide-ranging effects it has on many body systems, the symptoms of the perimenopause can sometimes be difficult to recognise at first. Perimenopause symptoms vary significantly between individuals. The table below summarises the most common symptoms that women experience.
| Symptom | Impact |
|---|---|
| Hot flushes | Often worse at night and impact sleep / work and other activities of daily living. |
| Erratic bleeding pattern | Bleeding can become irregular and heavier or lighter. |
| Acne or dry / thin skin and brittle nails | Adult-onset acne generally affects the jawline and neck.
Skin becomes thinner and drier increasing the risk of eczema and skin infections. |
| Sleep disturbance | Usually waking in the early hours and struggling to get back to sleep. |
| Low mood, anxiety and cognitive changes “brain fog” | Can affect many aspects of life at home and work. Premenstrual Syndrome (PMS) or Premenstrual Dysphoric Disorder (PMDD) can worsen. Brain fog can feel frustrating but generally improves with time. |
| Low libido | Can affect relationships and self-confidence. It is multifactorial and not always just due to hormonal changes. Other factors such as mid-life stressors, time constraints and fatigue all play an important role. |
| Genito-urinary Syndrome of the Menopause (GSM). | This is a condition that encapsulates the different issues that can happen around the vaginal and urinary tract area. Women can start to suffer with recurrent urinary tract infections, vaginal dryness and prolapse symptoms. |
| Heart palpitations | As oestrogen levels reduce, some women can develop palpitations. It is important to discuss these with a health professional; sometimes further tests are required to ensure they are not a cause for concern. |
| Weight gain | On average, women may gain around 1.5kg per year during perimenopause, with weight gain often accumulating around the middle. This is due to a combination of hormonal, metabolic and lifestyle changes. |
| Joint aches and pains | Oestrogen can act as a natural anti-inflammatory so as levels reduce, joints can become inflamed. Collagen loss weakens connective tissues increasing the risk of sprains and muscle strains. |
| Increased headaches or migraines | Erratic fluctuations and the eventual decline of oestrogen and progesterone affect brain chemicals and pain thresholds. |
What do we mean by lifestyle changes?
The six pillars of lifestyle medicine are key to improved health and wellbeing at any stage of life. However, for women going through the perimenopause, focusing on small changes within these areas can significantly reduce troublesome symptoms related to hormone fluctuations. These pillars include nutrition, physical activity, sleep, stress management, social connection and reducing harmful habits.

Fig 2: The components of lifestyle medicine. Source: Arora et al (2023). Frontiers in Nutrition
What are non-hormonal treatments?
For women not wishing to take hormones, there are several options that can help.
With regard to hot flushes, a newer oral medication called Fezolinetant (VEOZA) has recently been licensed in the UK. It is currently only available privately, but it is hoped it will become available on the NHS in due course. It can be effective at reducing hot flushes and consequently improving quality of life. Other medications that can help include Clonidine, Venlafaxine, Pregabalin and some antidepressants. Cognitive Behavioural Therapy (CBT) can also be extremely effective and is well worth exploring.
For acne and other skin changes, emollients are important, as well as more specific treatments such as oral antibiotics, a medication called Spironolactone and retinoid creams such as Adapalene.
Mood changes may respond well to CBT and lifestyle adjustments; some women might also require antidepressants. Low libido is often multifactorial and may require addressing several contributing factors such as time constraints, mid-life stressors and fatigue. Psychosexual counselling can be helpful. Vaginal lubricants are useful for Genito-Urinary Syndrome of the Menopause (GSM).
Once palpitations have been properly investigated and are not thought to be due to an underlying cardiac condition, medications such as beta blockers or addressing any underlying anxiety can help. Pain relief, physiotherapy and muscle strengthening can help with musculoskeletal symptoms. There are also many non-hormonal medications used to treat migraine, both to relieve acute attacks and to prevent further episodes. For some women, migraines are clearly linked to hormonal fluctuations and in these situations hormonal treatments can be useful.
What are hormonal treatments?
Hormone treatments aim to replace the oestrogen levels that have declined, therefore stabilising hormone fluctuations and improving the symptoms described above. There are many different options and combinations, so decisions around treatment should be individualised, as what works for one woman does not necessarily work for someone else.
It can also take time to find the right treatment, as any change may take around three months to take full effect. There are several different ways of administering HRT, and this has been covered in a previous newsletter.
Current approaches to menopause management broadly align with guidance from the National Institute for Health and Care Excellence (NICE).
What about contraception?
Despite hormonal fluctuations, women may still require contraception until the age of 55 years unless menopause has been confirmed. Some women can use the oral contraceptive pill until the age of 50 years, and there are newer pills that contain body-identical oestrogen (i.e. the same as that produced naturally by the body).
For other women, HRT may be more appropriate. It is important to remember that not all HRT treatments provide contraception, so this needs to be considered when prescribing HRT in women under the age of 55 years.
Are there longer-term considerations of the menopause?
While many treatment options focus on relieving troublesome symptoms, more recent evidence has highlighted the potential longer-term benefits of oestrogen. These include reducing the risk of osteoporosis and fragility fractures, as well as benefits for the heart and wider cardiovascular system.
Healthy women who start HRT soon after the menopause and continue for up to 10 years appear to have a reduced risk of heart disease and dying from heart-related causes.
There may be a slight increase in some types of ovarian cancer; however, the absolute risk is small, equating to around one extra case per 1,000 HRT users. In terms of breast cancer, unopposed HRT (oestrogen only) is associated with little or no change in risk, whereas combined HRT can be associated with a small increased risk when taken for more than five years.
The evidence regarding dementia risk and HRT has previously been conflicting. However, a recent review (December 2025) found no evidence that HRT either increases or decreases dementia risk in postmenopausal women.
The British Menopause Society also provides detailed guidance on the safe and effective use of hormone replacement therapy.
Moving forward…
Hormone fluctuations at any time in life can be challenging. Not everyone is affected, but if you are struggling with any of the symptoms described above, please do get in touch and speak to a health professional who can help you navigate this stage of life.
For many women, lifestyle adjustments are sufficient; for others, more tailored treatment (whether hormonal or non-hormonal) is appropriate. If your symptoms are affecting your quality of life, please speak to one of our GPs – we are here to support you.
References:
Arora et al (2023). Diet and lifestyle impact the development and progression of Alzheimer’s Dementia.
Front. Nutr. 10:1213223.
Melville et al (2025). Menopause hormone therapy and risk of mild cognitive impairment or dementia: a systematic review and meta-analysis. The Lancet Healthy Longevity. Vol 6, Issue 12, 100803.
About the author

BSc (hons) MBChB (hons) MRCP MRCGP DFSRH PPMC
Certified Menopause Specialist
“I believe in evidence-based, holistic care that supports women through every stage of life, particularly during the menopause.”
I am a GP with a specialist interest in women’s health and the menopause, and I am a Certified Menopause Specialist with the British Menopause Society. I provide evidence-based, individualised care to support women through perimenopause and menopause, taking time to consider symptoms in the context of overall health, lifestyle, mental wellbeing and long-term risk.
I enjoy working across all aspects of general medicine and take a holistic approach to patient care, combining lifestyle and dietary advice with appropriate medical treatments where needed. Supporting women to feel informed, confident and well supported during the menopause is a central part of my clinical practice.
I moved to Wiltshire in 2017 and now work as an NHS GP, alongside caring for private GP patients at Sloane Street Surgery’s Marlborough branch.